
Stem cell therapies have emerged as a promising frontier in the realm of regenerative medicine, offering innovative solutions for a diverse range of medical conditions. While the potential of these therapies is vast, their effectiveness is intrinsically tied to a multitude of crucial factors. In this comprehensive exploration, we will delve deep into the fundamental elements that influence the curative effect of mesenchymal stem cell (MSC) treatments. Furthermore, we will dissect the roles played by cell quality, injection route, optimal dosage, and treatment timing in the realm of stem cell therapy.
Understanding Cell Quality
Cell quality plays a pivotal role in determining the success of stem cell therapies. When discussing cell quality, we are referring to the biological potency of a unit or single cell. Essentially, the higher the potency, the better the cell quality. But what exactly is biological potency?
Biological potency, often referred to as bio-efficacy, is a multifaceted notion encompassing two critical facets: strength and effect. While strength relates to the concentration of the treatment, effect pertains to the outcomes achieved at a given strength. To illustrate this concept, let us consider two hypothetical individuals, A and B. A possesses the capability to move 2 tons of bricks daily but can compose only one SCI English sentence within the same timeframe. Conversely, B can transport 1 ton of bricks per day but can produce three SCI English sentences daily. In this scenario, A is more effective at moving bricks, while B exhibits greater efficiency in writing sentences. The concept of efficacy extends beyond stem cell therapies, finding utility in the evaluation of pesticides, drugs, and various biological realms.
In the context of stem cell therapies, biological efficacy assumes a distinct character predicated on the specific indication under consideration. For instance, MSCs manifest both immunosuppressive and angiogenesis-promoting properties, each wielding relevance in the treatment of distinct diseases. Consequently, different biological efficacy indicators are mandated for varying therapeutic applications. However, the current landscape of MSC research remains entrenched in a broader context, necessitating a preliminary focus on the factors underpinning general cell quality.
Several parameters serve as barometers of MSC quality, and these encompass cell viability, donor characteristics, clonogenic ability, cell size, immunosuppressive capacity, and cytokine secretion. In this section, we shall offer a succinct exploration of cell viability and donor characteristics – two pivotal determinants of cell quality:
- Cell Viability: Cell viability constitutes a pivotal facet of cell quality. In essence, cell viability quantifies the percentage of MSCs that retain their vitality before introduction into the patient’s body. Despite its paramount importance, the aspect of cell viability is regrettably often marginalized. Clinical studies divulge a gamut of cell viability rates, oscillating between 70% and upwards of 95%. Astonishingly, a plethora of foreign research articles cite cell viability rates falling short of the 90% threshold. This underscores the critical need to disabuse oneself of the notion that foreign-sourced stem cells inherently exhibit superior quality. The salient importance of cell viability can hardly be overstated, as the survival and functionality of MSCs within the patient’s body are the sine qua non for therapeutic efficacy.
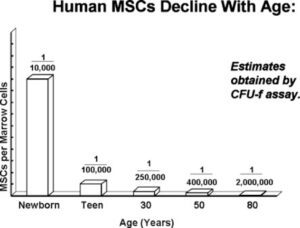
- Donor Characteristics: The characteristics of the donor, particularly age, exert a profound influence on the quality of MSCs. Youthful donors tend to yield MSCs characterized by elevated viability, heightened proliferative potential, and enhanced antioxidant capabilities – attributes that collectively augment their therapeutic potential. Moreover, the source of MSCs, ranging from umbilical cord, cord blood, placenta, deciduous teeth pulp, bone marrow, to fat, constitutes another pivotal variable shaping their quality. Intriguingly, advancing age bestows diminished quantities of MSCs in the bone marrow, making younger sources – such as umbilical cord and cord blood – particularly enticing. It is noteworthy that the gender of the donor can also influence certain functional properties of MSCs, with studies suggesting gender-based differences in immunosuppressive capacity.

About the Clinic
